What does Prioritisation station in MRCOG exam implies?
Prioritisation is a common formidable station for MRCOG part 3 exam which also is an essential component for MTI (Medical Training Initiative) and ST (Specialty Training O&G) interviews .
The idea underpinning here is to establish how confidently you can steer through either a labour ward board, a gynaecology pre-operative theatre list, GP letters for consultations, or any similar activity employing your managerial and leadership capabilities, other than your applied clinical knowledge.
Metaphorically, it’s your ship and you need to make sure everybody aboard sails through, without harm, taking alongside team members.
Considerations
- Are you able to demonstrate leadership skills?
- Are you prioritising patient well enough, based on available resources and expertise?
- Are you compromising on patient safety anywhere?
- Do you understand your strengths and limitations well enough?
- Do you understand limitation at an organisational level working in a team dynamics?
Analysing
See yourself being in that situation and then run through the given scenario in your head. This helps you to perform as if you are in a real-life situation. Simultaneously, answer the above questions while formulating your priority order and the management plan.
Be aware of the pitfalls and traps laid out in the prioritisation scenario. Try not answer just by eyeballing the labour ward board as you can encounter terminologies like placenta previae, meconium stained liqour, very preterm with SROM, Jeehova’s witness background, etc which might alarm you and get adrenaline pumping, this can blur your sensible decision making capacity and there you fall in the trap.
Always read the station thoroughly and in complete prior to gathering your thoughts.
Action plan
Top tips:
During reading time, it’s a good idea to apply some structure or framework wherein you can put applied clinical knowledge and also use it as a reference while having a preparing for a conversation in the ‘SBAR’ format.
I have suggested one such, which I find useful:-
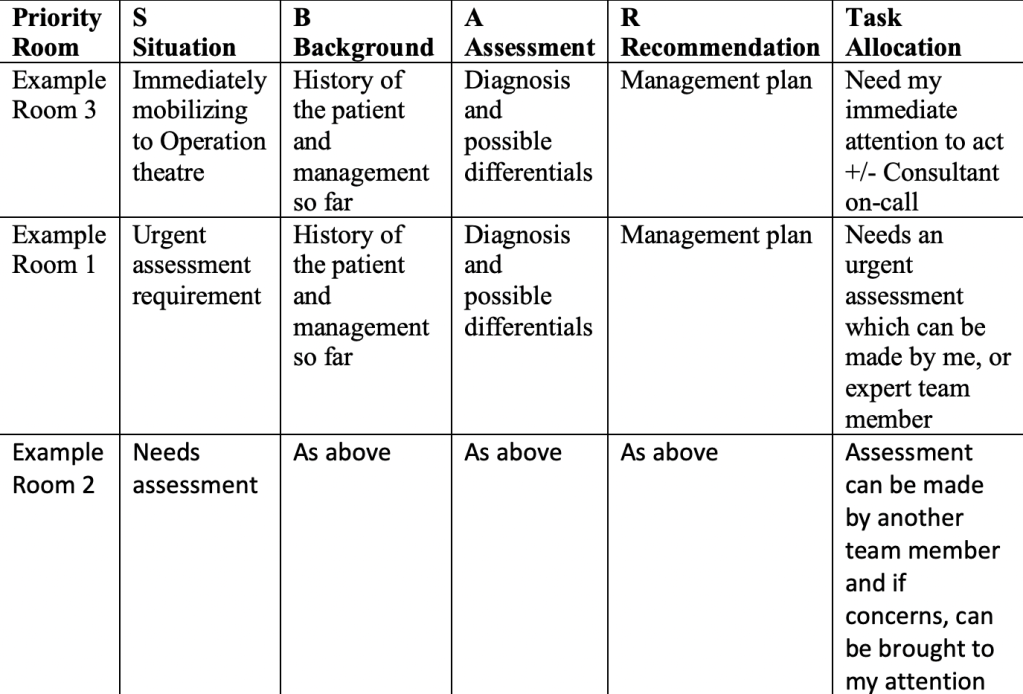
I have used imaginary scenarios above to demonstrate one such framework, where you can add your thoughts while deciding for prioritisation, management and task allocation. This all will be available in one page and you can refer back to it as going through the station.
Undoubtedly, there will be a need to divide priority for a review or an action into immediate, urgent, semi-urgent, or elective situations from the given scenarios. There might be seemingly overlapping situations which will require justifying priority by you. Finally, during task allocation be mindful of situations that can be managed only by you as an expert and no one else, like performing a cesarean, conducting an instrumental delivery, repairing a complex tear.
Keeping it simple, divide your situation based on need of an action and assessment/review. Furthermore, differentiate them based on things that can be performed only by you and no one else. Similarly, patient’s assessment which are urgent and requires either your expertise or can be reviewed by a senior midwife or anaesthetist. Then allocate tasks to remaining team members bearing their roles and training in mind.
The above discussion although seems more relevant in the context of labour ward prioritisation but can be pretty much extrapolated in gynaecology prioritisation, something which I will potentially re-visit at a later stage.
Hopefully, this mellows down your apprehension with prioritisation stations.

Leave a comment